Share this:




 DEAR MAYO CLINIC: How is endometriosis diagnosed? I’m 20 and have painful, heavy periods. Lately, I also have terrible lower back pain during my period. If it is endometriosis, how is it treated? I’m worried this could affect my fertility down the road.
DEAR MAYO CLINIC: How is endometriosis diagnosed? I’m 20 and have painful, heavy periods. Lately, I also have terrible lower back pain during my period. If it is endometriosis, how is it treated? I’m worried this could affect my fertility down the road.
ANSWER: Endometriosis could be causing your symptoms, but other conditions can cause painful periods, too. See your health care provider for an evaluation. If you have endometriosis, treatment is available. This condition sometimes can affect fertility; however, many women with minimal or mild endometriosis have no trouble having a baby.
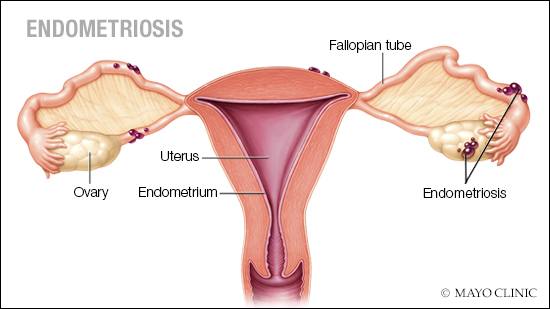
In endometriosis, tissue that normally lines the inside of the uterus, the endometrium, grows outside the uterus. Endometriosis most commonly involves the ovaries, fallopian tubes and tissue lining the pelvis. Rarely, endometrial tissue may spread beyond pelvic organs.
Pain is the most common symptom of endometriosis. Often, pain and cramping begin several days before a period starts and may last several days into a period. Although many women have discomfort during their periods, women with endometriosis typically describe severe menstrual pain that’s far worse than usual. They also tend to report that the pain increases and occurs more often over time.
Other symptoms may include heavy periods, pain during or after sex, lower back pain, abdominal pain, and pain with bowel movements or urination, especially during your period. Endometriosis also can cause diarrhea, constipation, fatigue, bloating and nausea, particularly during periods.
If your health care provider suspects endometriosis based on your symptoms, she or he may perform a pelvic exam to check for abnormalities, such as cysts on your reproductive organs or scars behind your uterus that could be a result of endometriosis. An ultrasound of your reproductive organs may be recommended. Although an ultrasound cannot show superficial forms of the endometrial tissue, it can reveal cysts associated with endometriosis and sometimes nodular endometriosis as well.
In some cases, the results of a pelvic exam and an ultrasound, coupled with an individual’s symptoms, are enough to suggest a diagnosis of endometriosis. But, in other situations, a surgical procedure called laparoscopy may be necessary. This is also the only way to make a definitive diagnosis.
During laparoscopy, a surgeon inserts a slender viewing instrument through a small incision near the navel to look for endometrial tissue outside the uterus. Abnormalities are biopsied and sent to a lab to confirm the diagnosis. Laparoscopy can provide your health care provider with information about the location, extent and size of endometriosis, while allowing for removal of the endometrial tissue at the same time.
Treatment for endometriosis can involve medication and surgery. Medication such as pain relievers and hormonal therapy can ease endometriosis symptoms, but it won’t necessarily change the underlying disease. Surgery to remove endometrial tissue outside the uterus is the only way to eliminate that tissue. Unfortunately, sometimes endometriosis can recur after surgical treatment.
Some health care providers suggest a hysterectomy — removal of the uterus — to treat endometriosis. But, again, that doesn’t eliminate the tissue that’s developed outside the uterus, and it does eliminate the possibility of future pregnancies. In addition, recent evidence indicates that women younger than 35 who have a hysterectomy for endometriosis have an increased risk of heart disease as they get older. Because of these factors, a hysterectomy typically is recommended for endometriosis only when there are specific reasons for the procedure, such as relieving heavy bleeding or eliminating pain that starts in the uterus.
About one-third to one-half of women who have endometriosis experience problems with infertility. But the exact connection between endometriosis and infertility isn’t clear. Part of the problem seems to be that if endometrial tissue or scarring is located in or around the fallopian tubes, it may hamper an egg’s ability to reach the uterus. Endometriosis also may damage the egg and the sperm, making conception more challenging. However, many women with endometriosis go on to have successful pregnancies. — Dr. Tatnai Burnett, Obstetrics and Gynecology, Mayo Clinic, Rochester, Minnesota


