-
Health & Wellness
#ThrowbackThursday: Innovation In Hospital Care
Share this:





This article first appeared Oct. 5, 1957 in the publication Mayovox.
Some time next month the Rochester Methodist Hospital expects to have ready for occupancy its new 12-bed constant observation unit, the “circle hospital” which has been built to the rear of the main building and connects to the hospital proper on second floor.
More than three years of study and planning preceded construction of the unit. The period of trial during which there will be intensive study of efficiency of operation, staffing patterns and methods of patient care may take another three years.
Grants from the Ford and Hill Foundations have provided funds for construction of the unit. There is the possibility of other grants to finance a study of its operation.
Hospital administrator Harold C. Mickey looks on the project as “a unique opportunity to test a new approach to patient care that might affect hospital construction before we proceed with a building program.”
The months of preliminary study included a survey of patients in all hospitals serving Clinic patients, and several detailed studies of the care of the seriously ill patient.
Key Need
These studies, says Mickey, “gave us some answers in regard to space and equipment needed to enable nursing personnel to work at peak efficiency. When we asked ‘what is the key need of the nurse in caring for a group of seriously ill patients,’ the answer seemed to be ‘the ability to see all of the patients in the unit all the time.’”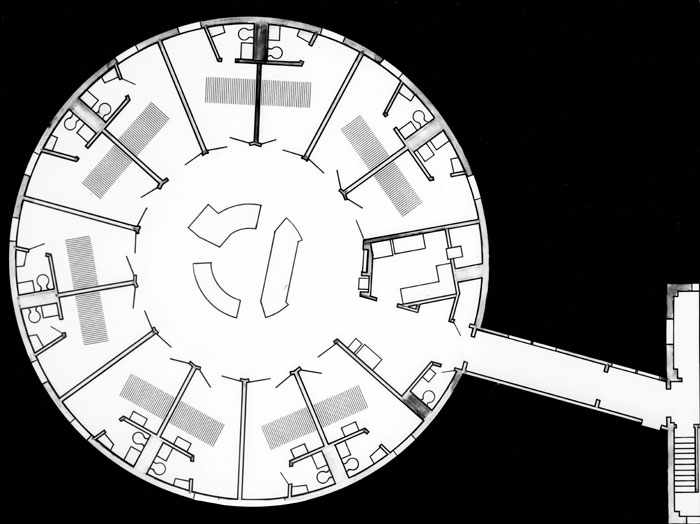
These answers were incorporated in plans for the new 12-bed unit. The patients’ rooms are placed in a circle with the nurses station in the center. Through the glassed upper half of the doors to the rooms a nurse at her station can see every patient in the unit. Distance from nurses station to the bedside of any patient is 15 feet.
The rooms are large enough for convenient care of the patient and placement of special equipment and apparatus. The lavatory area of each room will also serve as a nurse’s sub-utility room in which will be kept all equipment and supplies needed for the care of that particular patient.
Outlets for oxygen, suction (three types), air and electricity are built into each room. The area will be air conditioned with temperature and humidity controls in each room.
Thought has been given to even so seemingly minor a detail as the energy expended to open and close a door. Doorways to hospital rooms must be wide enough to admit a bed and the large door is heavy. Rooms in the new unit have double doors and one section only need ordinarily be used.
Decorators will select interesting but restful wall colors and window draperies. Shades will also be provided on the doors to give privacy when this is desired. Lighting facilities will provide four stages of illumination from the minimal “night light” to maximal light needed for a physician’s examination.
Many Contribute
Several organizations and individuals have made important contributions in planning this new unit. George Huvos and his associates in the Materials Handling Department of IBM carried out studies which will lead to better utilization of nursing services. The research department of another organization has made most significant contributions toward ease of moving the patient into and out of the unit. A special research team will carry out studies on devices to record automatically temperature, blood pressure, respiration and pulse rate.
A room for a resident physician who will be immediately available during the night hours will be located adjacent to the new unit. A room has also been provided in which the patient’s relatives may talk with physicians. The nurses' station will have direct communication with two regular hospital stations and with the pharmacy and central supply room.
While the present unit has facilities for 12 patients, further studies may show that this is not the optimal number, planners state.
Several members of the Clinic staff served on the committee which worked with Mr. Mickey, hospital personnel and Ellerbe and Company in planning the unit. These included Drs. O.T. Clagett, O.H. Beahrs, H.W. Schmidt, and R.A. Theye and E. H. Weld. Now a new committee will constructively criticize and evaluate the operation of the unit. This committee includes Drs. F. R. Keating, D. T. Carr and B.M. Black, Robert Gage and Madelyne Sturdavant, who is specially trained in research methods and has been employed by the hospital to assist the medical investigating team and carry out the studies.
First use of the unit will be for the critically ill patient. It may also be tested with the moderately ill, the convalescent and the preoperative patient.
May Be Answer
The new circle unit may help answer two problems which plague hospitals and patients alike: the spiraling cost of hospital care and the shortage of nursing personnel.
“What we are trying to do,” says Mr. Mickey, “is to learn how to provide the patient with the best possible care at the lowest possible cost. This means we must find the most efficient way in which to utilize space, equipment and nursing services. Whether circular construction is one answer is what we hope to find out during the coming months.
“We aren’t forgetting, of course, that ‘best possible’ patient care involves more than economics. The human quality of kindliness in the care of the sick will always be the primary need in any hospital.”
Related Articles


