-
Cancer
Tuesday Q and A: Many factors determine treatment plan for rectal cancer
Share this:




DEAR MAYO CLINIC: I often hear about colon cancer, but not a lot about rectal cancer. How is it diagnosed, and is it treatable?
ANSWER: Rectal cancer is cancer that occurs in the last several inches of the colon, called the rectum. The primary treatment for rectal cancer is surgery and — depending on how advanced the cancer is — may also include radiation therapy and chemotherapy.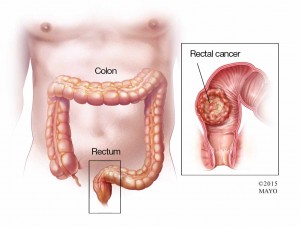 If rectal cancer is caught early, the long-term survival rate is about 85 to 90 percent. Those numbers decline sharply if rectal cancer has spread to lymph nodes.
If rectal cancer is caught early, the long-term survival rate is about 85 to 90 percent. Those numbers decline sharply if rectal cancer has spread to lymph nodes.
Most rectal cancers begin as small, noncancerous growths of cells called polyps. Removing polyps before they become cancerous can prevent rectal cancer. That’s why timely colon cancer screening with a colonoscopy is important. Guidelines generally recommend that screening should begin at age 50. Your doctor may recommend more-frequent or earlier colon cancer screening if you have other risk factors, such as a family history of colorectal cancer.
Many people with rectal cancer experience no signs and symptoms in early stages of the disease. Signs and symptoms in later stages may include rectal bleeding (often bright red); a change in bowel habits; abdominal discomfort; rectal pain; persistent urge to have a bowel movement; and/or a sensation of fullness along with painful, ineffective straining to pass stool.
Any first episode of rectal bleeding should be evaluated to determine the cause. Many people may attribute rectal bleeding to common conditions such as hemorrhoids, but unless you have a known diagnosis of hemorrhoids you should pursue medical evaluation as early as possible to rule out the presence of a polyp or rectal cancer.
An important step in evaluating any rectal bleeding is a digital rectal exam. To do this, your doctor will insert a lubricated, gloved finger into the lower part of your rectum to check for anything that feels unusual.
Other tests may be done in addition to confirm the diagnosis and determine how advanced the cancer is (its stage). A colonoscopy allows the doctor to view the entire colon. Polyps or tissue samples can be removed or biopsied. A computerized tomography (CT) scan or X-ray can determine whether the cancer has spread. Other tests, such as endoscopic ultrasonography or magnetic resonance imaging (MRI), can help determine how deeply the cancer has penetrated the wall of the rectum and if lymph nodes are involved.
Many factors influence the treatment plan. If the tumor hasn’t grown through the rectal wall and lymph nodes haven’t been affected, the cancer is considered to be very early (stage I). A tumor that has invaded into or slightly through the wall of the rectum, but not spread to lymph nodes, is stage II. If nearby lymph nodes are involved, it’s stage III. Cancer that has spread to other areas is stage IV.
Surgery is the most common treatment for all stages of rectal cancer. The type of surgery is determined by the tumor’s location and whether the muscle rings at the end of the rectum (anal sphincters) — which normally control release of stool — are involved.
For cancer that’s grown into or through the rectum, the surgeon may recommend removing (resecting) the part of the rectum with cancer along with a margin of healthy rectal tissue near the cancer. Nearby lymph nodes are removed and checked for cancer.
When possible, healthy remaining portions of the rectum and colon are reconnected. If reconnection isn’t possible, then creating a permanent opening (stoma) from part of the remaining bowel through the wall of the abdomen may be necessary. This is called a colostomy, and allows waste to pass out of the body into an external appliance.
In addition to surgery, locally advanced rectal cancer generally is treated with radiation and chemotherapy. Chemotherapy and radiation generally are used when the cancer has spread to nearby lymph nodes or has clearly grown through the wall of the rectum.
If cancer has not spread to other areas of the body, chemotherapy and radiation typically are done before surgery to shrink the tumor and improve the ability to completely resect it. Combined chemotherapy and radiation therapy generally is recommended before surgery for stage II and III rectal cancers, with more chemotherapy after surgery.
Given the seriousness of advanced rectal cancer, it’s important to see your doctor at the first sign or symptom, particularly rectal bleeding, change in stool size or character, or persistent rectal discomfort . — Robert Cima, M.D., Colon & Rectal Surgery, Mayo Clinic, Rochester, Minn.


