-
COVID-19
What’s the latest on monoclonal antibody therapies to treat COVID-19?
Share this:





As COVID-19 continues to evolve and mutate quickly, so do treatment options. While the best ways to prevent the spread of COVID-19 are vaccinations and booster vaccinations, several authorized treatments and preventive drugs, including monoclonal antibody therapies, are used to treat patients at different stages.
Monoclonal antibody therapies are laboratory-produced proteins created to bind to SARS-CoV2, the virus that causes COVID-19, and prevent it from attaching to human cells. While these therapies have been used to treat COVID-19 since late 2020, some treatments have become less effective or ineffective as COVID-19 mutates.
The monoclonal antibody therapies authorized for emergency use by the Food and Drug Administration (FDA) to treat COVID-19 are:
- Bamlanivimab plus etesevimab.
- Casirivimab plus imdevimab (known as REGEN-COV).
- Sotrovimab.
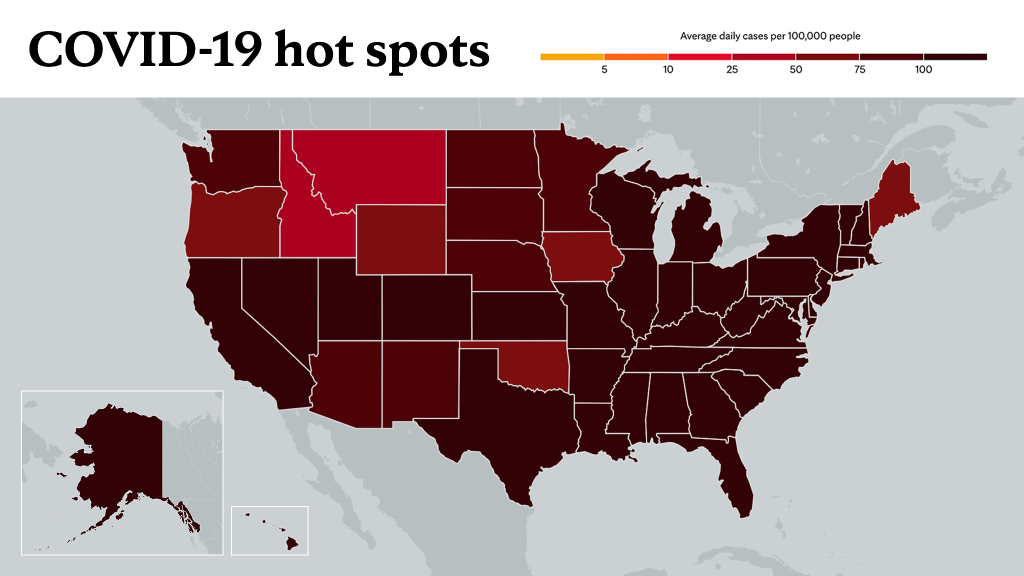
However, only sotrovimab may be effective against the newest variants of COVID-19, including omicron. As of Jan. 8, the omicron variant accounted for 98.3% of COVID-19 infections, according to the Centers for Disease Control and Prevention (CDC). Bamlanivimab plus etesevimab and casirivimab plus imdevimab are ineffective against omicron and are no longer used today.
In addition, the FDA issued an emergency use authorization in December 2021 for the monoclonal antibody therapy combination of tixagevimab plus cilgavimab, known as EvuSheld, for preexposure prophylaxis to prevent COVID-19 infection in certain people deemed high-risk and unable to develop immunity from vaccination, such as people who are immunocompromised and those who are allergic to the vaccinations.
Here's more information on the two monoclonal antibody therapies that the FDA recommends and criteria for their use:
Sotrovimab
Sotrovimab is authorized to treat mild to moderate COVID-19 in patients at high risk of hospitalization and disease progression. These patients need to be 12 and older and weigh at least 88 pounds.
To be treated with sotrovimab, patients must:
- Test positive for COVID-19.
- Begin treatment within 10 days of the start of symptoms.
- Not require oxygen supplementation.
- Not be hospitalized for COVID-19.
This therapy is not indicated for preexposure or postexposure prophylaxis.
EvuSheld
EvuSheld is authorized to prevent COVID-19 before exposure for those 12 and older who weigh at least 88 pounds.
To be treated with EvuSheld, patients must:
- Have a weakened immune system.
- Not be expected to respond to COVID-19 vaccination or not be able to get vaccinated for COVID-19 for medical reasons.
Along with the monoclonal antibody therapies, the FDA has granted emergency use authorization to two oral antiviral pills to treat mild to moderate COVID-19: nirmatrelvir tablets plus ritonavir, known as Paxlovid, and molnupiravir for high-risk patients. In addition, a three-day regimen of remdesivir, an FDA-approved antiviral drug, has been recommended for off-label use in outpatients at high risk of hospitalization.
"Therapies for COVID-19 continue to evolve, and depending on the clinical condition of a patient and their risk factors, they may be eligible for treatment with monoclonal antibodies or antiviral drugs," says Dr. Raymund Razonable, a Mayo Clinic infectious diseases expert. "But the best medicine is prevention. Efforts to recommend vaccination to as many people as possible is undertaken for the transmission of COVID-19 to decline so that people don't need to go to the hospitals to get these treatments."
As the omicron variant of COVID-19 continues its spread across the country, Mayo Clinic is refining its approach to effectively treat infected outpatients with monoclonal antibody and antiviral drug therapies. Treatment options are available across Mayo Clinic on an extremely limited basis.
A confluence of factors, including supply chain issues, and pauses and inconsistencies in distribution, have contributed to these treatment supply shortages. Also, a rapid rise in omicron infection rate across the country has affected transportation staff, which has contributed to these supply shortages. Due to scarcity of resources, patients should consult with their current health care provider to determine the best course of appropriate treatment.
____________________________________________
Information in this post was accurate at the time of its posting. Due to the fluid nature of the COVID-19 pandemic, scientific understanding, along with guidelines and recommendations, may have changed since the original publication date.
For more information and all your COVID-19 coverage, go to the Mayo Clinic News Network and mayoclinic.org.
Learn more about tracking COVID-19 and COVID-19 trends.